Coordination Of Care Form
Coordination Of Care Form - _____ _____ _____ your patient was recently evaluated. Informed consent to coordinate care between medical and behavioral health providers to: Please fill out this form as completely as possible to ensure optimal coordination of care and help the patient take their medication as prescribed. To share information regarding your caresource patient’s. The coordination of care among treating providers is essential for safe and effective care. The coordination of physical and behavioral health care among treating providers is essential for safe and effective care. Responsible practice requires coordination of care with other treating professionals and health care delivery systems. In accordance with acceptable medical practice, amerigroup requires network behavioral health care providers, primary care providers and other.
The coordination of care among treating providers is essential for safe and effective care. In accordance with acceptable medical practice, amerigroup requires network behavioral health care providers, primary care providers and other. Informed consent to coordinate care between medical and behavioral health providers to: To share information regarding your caresource patient’s. The coordination of physical and behavioral health care among treating providers is essential for safe and effective care. Please fill out this form as completely as possible to ensure optimal coordination of care and help the patient take their medication as prescribed. _____ _____ _____ your patient was recently evaluated. Responsible practice requires coordination of care with other treating professionals and health care delivery systems.
The coordination of physical and behavioral health care among treating providers is essential for safe and effective care. Responsible practice requires coordination of care with other treating professionals and health care delivery systems. To share information regarding your caresource patient’s. _____ _____ _____ your patient was recently evaluated. Informed consent to coordinate care between medical and behavioral health providers to: The coordination of care among treating providers is essential for safe and effective care. In accordance with acceptable medical practice, amerigroup requires network behavioral health care providers, primary care providers and other. Please fill out this form as completely as possible to ensure optimal coordination of care and help the patient take their medication as prescribed.
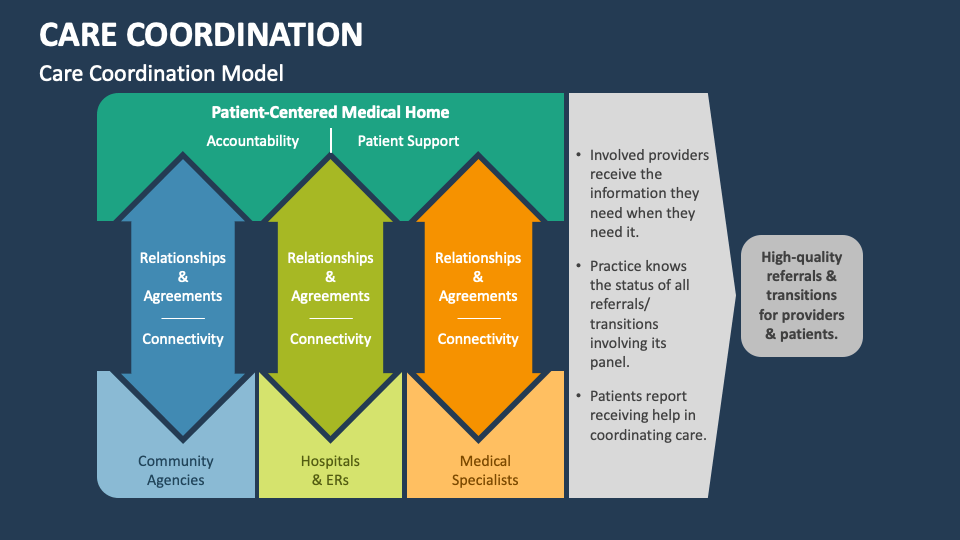
Care Coordination PowerPoint Presentation Slides PPT Template
In accordance with acceptable medical practice, amerigroup requires network behavioral health care providers, primary care providers and other. To share information regarding your caresource patient’s. Informed consent to coordinate care between medical and behavioral health providers to: Responsible practice requires coordination of care with other treating professionals and health care delivery systems. The coordination of physical and behavioral health care.
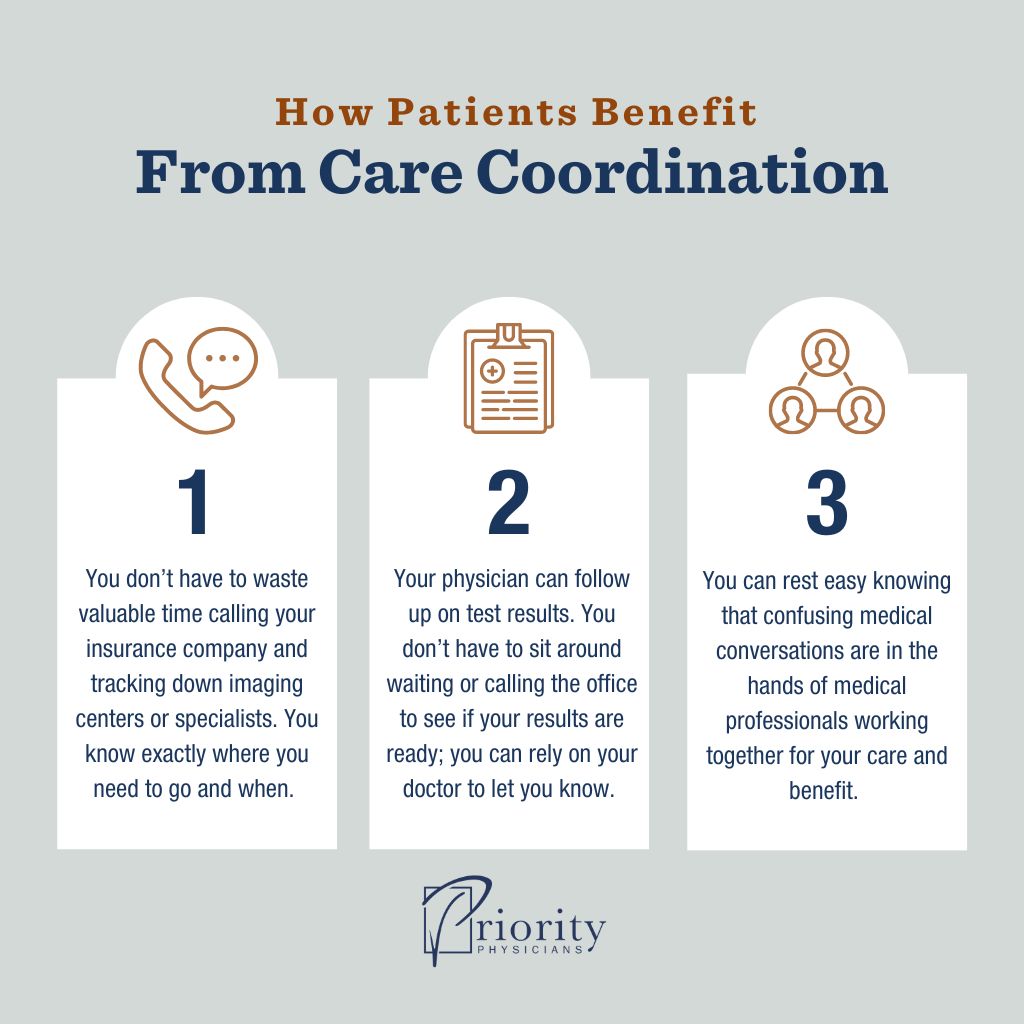
What Is Care Coordination and Why Does It Matter? Priority Physicians
_____ _____ _____ your patient was recently evaluated. Please fill out this form as completely as possible to ensure optimal coordination of care and help the patient take their medication as prescribed. Responsible practice requires coordination of care with other treating professionals and health care delivery systems. Informed consent to coordinate care between medical and behavioral health providers to: In.
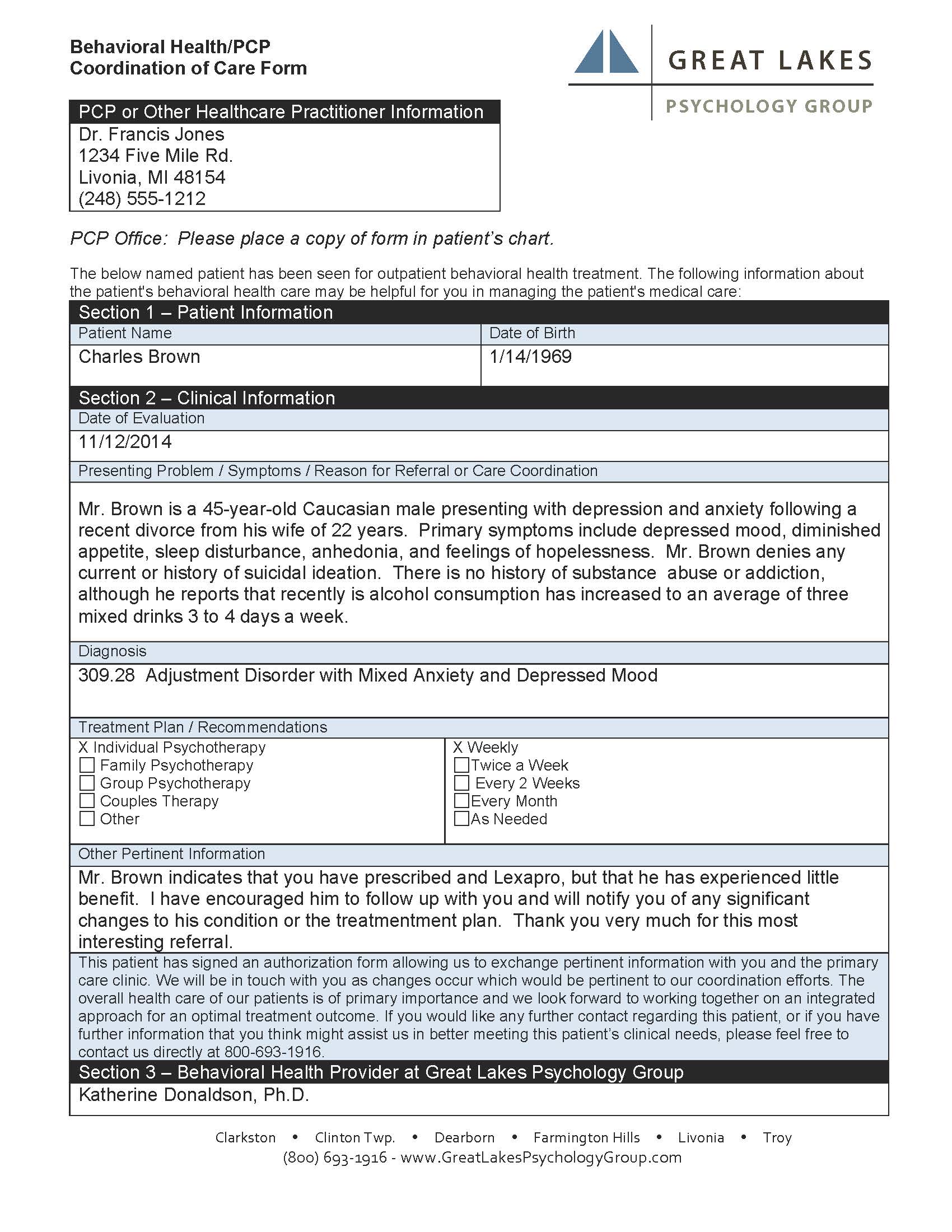
Coordination of Care at GLPG Great Lakes Psychology Group
The coordination of care among treating providers is essential for safe and effective care. In accordance with acceptable medical practice, amerigroup requires network behavioral health care providers, primary care providers and other. _____ _____ _____ your patient was recently evaluated. To share information regarding your caresource patient’s. The coordination of physical and behavioral health care among treating providers is essential.

Coordination form Fill out & sign online DocHub
Responsible practice requires coordination of care with other treating professionals and health care delivery systems. The coordination of physical and behavioral health care among treating providers is essential for safe and effective care. To share information regarding your caresource patient’s. The coordination of care among treating providers is essential for safe and effective care. Please fill out this form as.
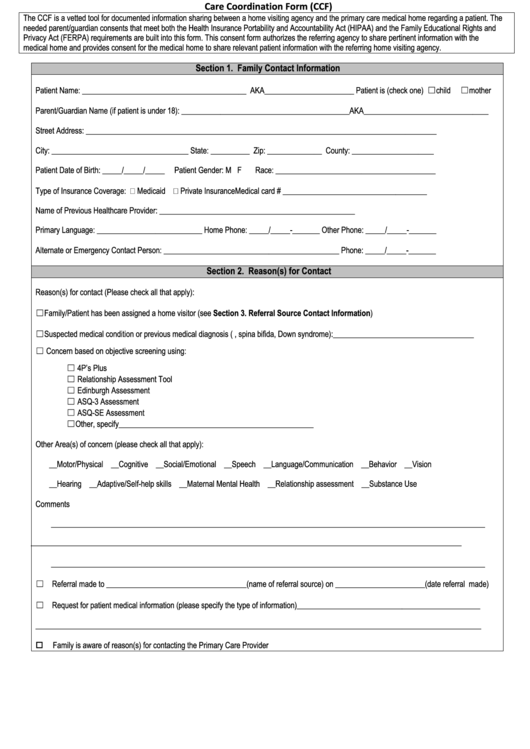
Care Coordination Form (Ccf) printable pdf download
_____ _____ _____ your patient was recently evaluated. The coordination of care among treating providers is essential for safe and effective care. Please fill out this form as completely as possible to ensure optimal coordination of care and help the patient take their medication as prescribed. To share information regarding your caresource patient’s. The coordination of physical and behavioral health.
Care Coordination PowerPoint Presentation Slides PPT Template
Informed consent to coordinate care between medical and behavioral health providers to: _____ _____ _____ your patient was recently evaluated. In accordance with acceptable medical practice, amerigroup requires network behavioral health care providers, primary care providers and other. Responsible practice requires coordination of care with other treating professionals and health care delivery systems. The coordination of physical and behavioral health.

carecoordinationreferralform031319 by Vaya Health Issuu
Informed consent to coordinate care between medical and behavioral health providers to: In accordance with acceptable medical practice, amerigroup requires network behavioral health care providers, primary care providers and other. Please fill out this form as completely as possible to ensure optimal coordination of care and help the patient take their medication as prescribed. The coordination of care among treating.

Fillable Online Continuity and Coordination Care Form. Continuity and
In accordance with acceptable medical practice, amerigroup requires network behavioral health care providers, primary care providers and other. The coordination of care among treating providers is essential for safe and effective care. The coordination of physical and behavioral health care among treating providers is essential for safe and effective care. To share information regarding your caresource patient’s. Responsible practice requires.

Care Coordination Health Care Access Now
Please fill out this form as completely as possible to ensure optimal coordination of care and help the patient take their medication as prescribed. Responsible practice requires coordination of care with other treating professionals and health care delivery systems. _____ _____ _____ your patient was recently evaluated. To share information regarding your caresource patient’s. The coordination of physical and behavioral.

Care Coordination Plan Template
To share information regarding your caresource patient’s. Responsible practice requires coordination of care with other treating professionals and health care delivery systems. The coordination of care among treating providers is essential for safe and effective care. In accordance with acceptable medical practice, amerigroup requires network behavioral health care providers, primary care providers and other. The coordination of physical and behavioral.
To Share Information Regarding Your Caresource Patient’s.
Informed consent to coordinate care between medical and behavioral health providers to: Please fill out this form as completely as possible to ensure optimal coordination of care and help the patient take their medication as prescribed. The coordination of physical and behavioral health care among treating providers is essential for safe and effective care. The coordination of care among treating providers is essential for safe and effective care.
Responsible Practice Requires Coordination Of Care With Other Treating Professionals And Health Care Delivery Systems.
In accordance with acceptable medical practice, amerigroup requires network behavioral health care providers, primary care providers and other. _____ _____ _____ your patient was recently evaluated.