Family Health History Form
Family Health History Form - Put a ü in the “yes”, “no” box for any health conditions you, your partner or your family members have now or have had in the. Is there anyone else on the maternal side of the family that has any birth defects, mental retardation, or any other health concerns not yet. Complete all the fields as best you can. Read the directions for each section —. Use the march of dimes family health history form and share it with your health care provider. The form does not have to be complete but every piece of information helps. What is your family health history? Family health history form fill out all pages of this form about you, your partner and your families.
Complete all the fields as best you can. Use the march of dimes family health history form and share it with your health care provider. Put a ü in the “yes”, “no” box for any health conditions you, your partner or your family members have now or have had in the. Is there anyone else on the maternal side of the family that has any birth defects, mental retardation, or any other health concerns not yet. Family health history form fill out all pages of this form about you, your partner and your families. What is your family health history? Read the directions for each section —. The form does not have to be complete but every piece of information helps.
Put a ü in the “yes”, “no” box for any health conditions you, your partner or your family members have now or have had in the. Read the directions for each section —. Complete all the fields as best you can. Is there anyone else on the maternal side of the family that has any birth defects, mental retardation, or any other health concerns not yet. Use the march of dimes family health history form and share it with your health care provider. What is your family health history? Family health history form fill out all pages of this form about you, your partner and your families. The form does not have to be complete but every piece of information helps.
Family Medical History Template
Put a ü in the “yes”, “no” box for any health conditions you, your partner or your family members have now or have had in the. Use the march of dimes family health history form and share it with your health care provider. Is there anyone else on the maternal side of the family that has any birth defects, mental.
Editable Medical History Form, Family Medical History Form , Medical
Put a ü in the “yes”, “no” box for any health conditions you, your partner or your family members have now or have had in the. Use the march of dimes family health history form and share it with your health care provider. Complete all the fields as best you can. Is there anyone else on the maternal side of.
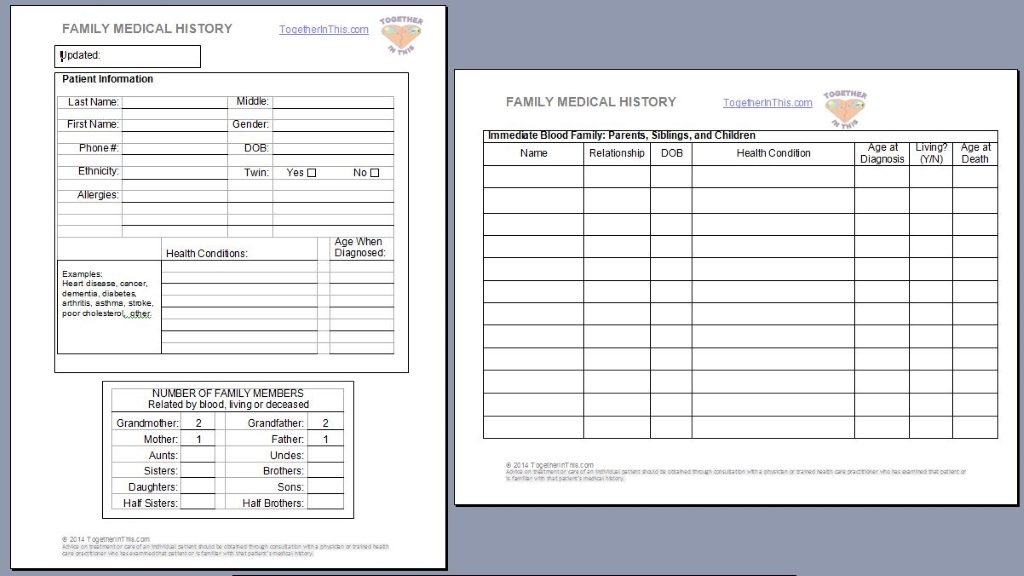
Family Medical History Form Together in This
The form does not have to be complete but every piece of information helps. Put a ü in the “yes”, “no” box for any health conditions you, your partner or your family members have now or have had in the. Read the directions for each section —. Family health history form fill out all pages of this form about you,.
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-03-scaled-e1617709269345.jpg)
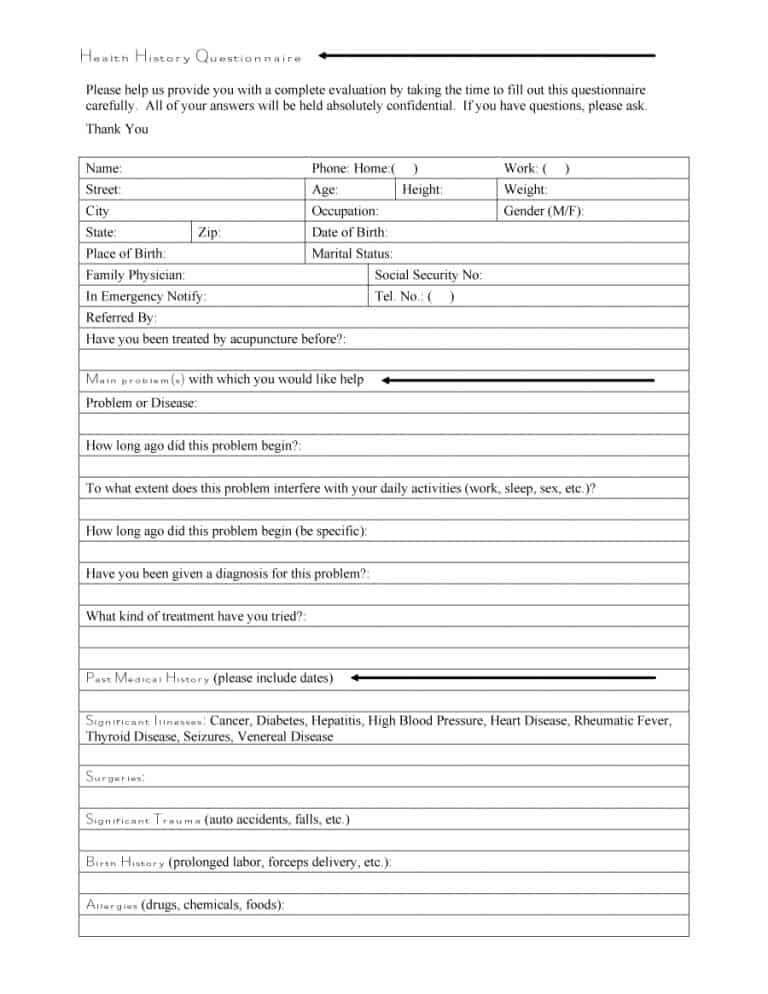
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
Use the march of dimes family health history form and share it with your health care provider. What is your family health history? Is there anyone else on the maternal side of the family that has any birth defects, mental retardation, or any other health concerns not yet. Read the directions for each section —. Family health history form fill.
Printable Family Medical History Form Template
Family health history form fill out all pages of this form about you, your partner and your families. Is there anyone else on the maternal side of the family that has any birth defects, mental retardation, or any other health concerns not yet. What is your family health history? The form does not have to be complete but every piece.
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-36-scaled.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
What is your family health history? Is there anyone else on the maternal side of the family that has any birth defects, mental retardation, or any other health concerns not yet. Complete all the fields as best you can. The form does not have to be complete but every piece of information helps. Read the directions for each section —.
Comprehensive Health History Template
Is there anyone else on the maternal side of the family that has any birth defects, mental retardation, or any other health concerns not yet. The form does not have to be complete but every piece of information helps. Family health history form fill out all pages of this form about you, your partner and your families. What is your.
Printable Family Health History Form Printable Forms Free Online
Put a ü in the “yes”, “no” box for any health conditions you, your partner or your family members have now or have had in the. Family health history form fill out all pages of this form about you, your partner and your families. What is your family health history? Is there anyone else on the maternal side of the.

Family History Medical Form medical form templates
Put a ü in the “yes”, “no” box for any health conditions you, your partner or your family members have now or have had in the. Read the directions for each section —. Complete all the fields as best you can. What is your family health history? Family health history form fill out all pages of this form about you,.
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-05-scaled.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
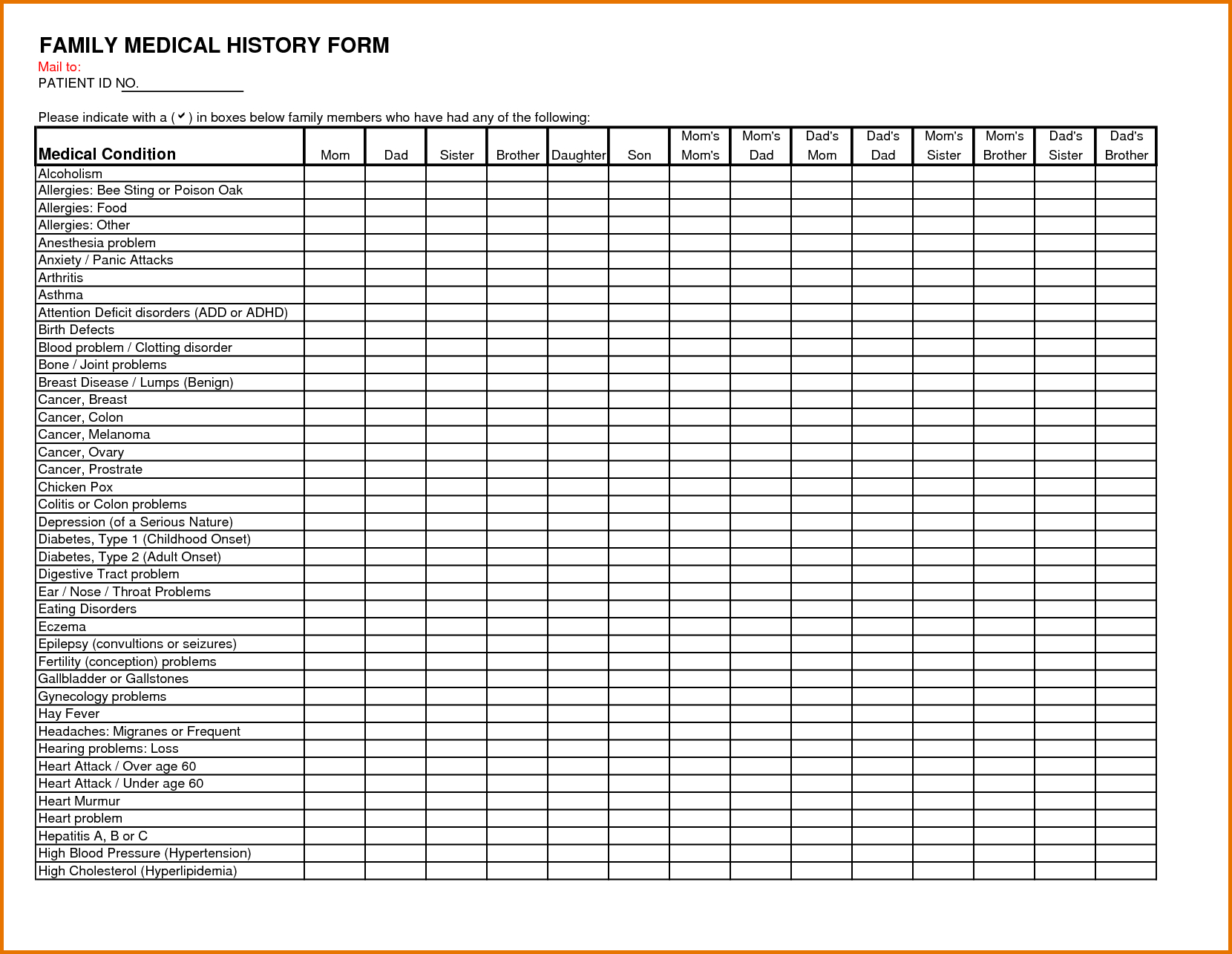
The form does not have to be complete but every piece of information helps. Read the directions for each section —. Put a ü in the “yes”, “no” box for any health conditions you, your partner or your family members have now or have had in the. Use the march of dimes family health history form and share it with.
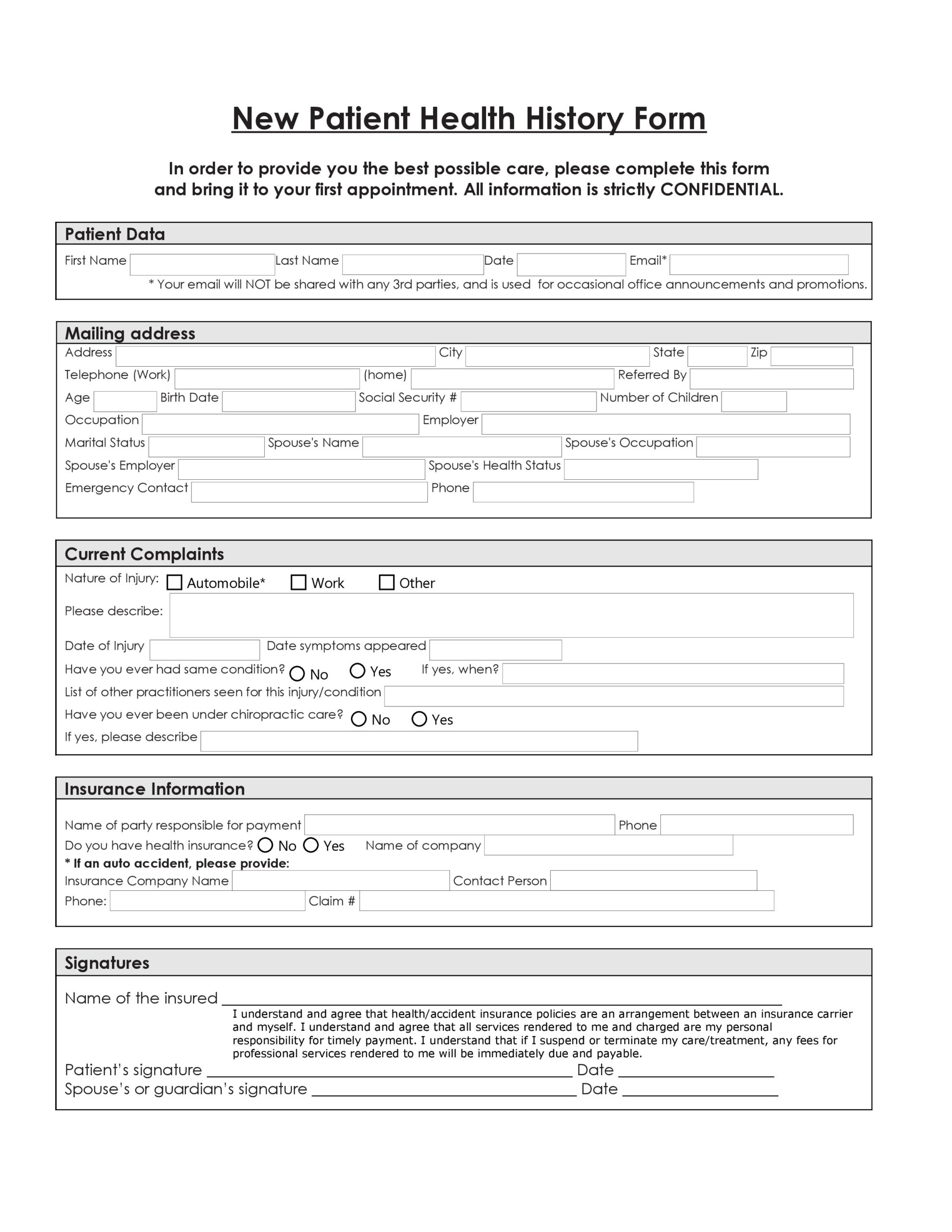
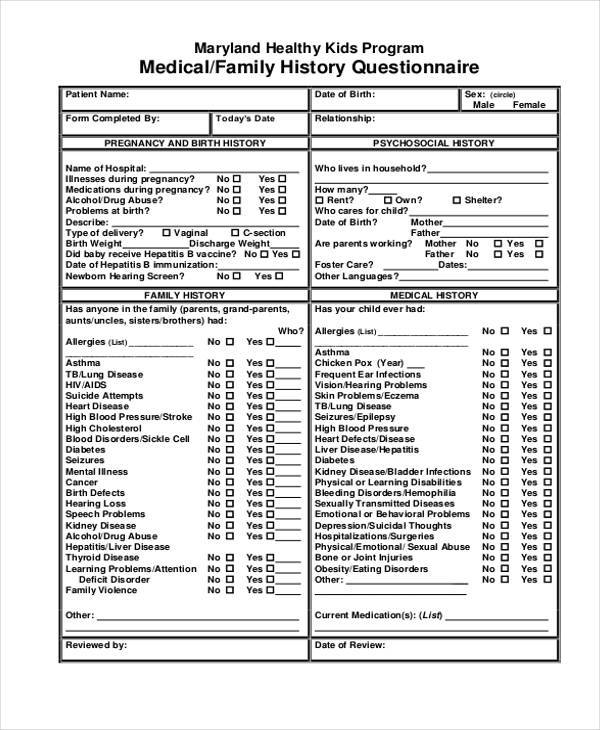
Complete All The Fields As Best You Can.
Read the directions for each section —. Family health history form fill out all pages of this form about you, your partner and your families. Is there anyone else on the maternal side of the family that has any birth defects, mental retardation, or any other health concerns not yet. Use the march of dimes family health history form and share it with your health care provider.
What Is Your Family Health History?
Put a ü in the “yes”, “no” box for any health conditions you, your partner or your family members have now or have had in the. The form does not have to be complete but every piece of information helps.